ABSTRACT
In August, 2009, Dr. E.C.Sreevalsan has put into practice his “New Concept”, that” errors of development of the Mullerian Tract ( Mullerian Dysgenesis ) could be corrected and made to grow on normal lines, after the age of 16 years (when growth spurt diminishes ) and become functional, by the use of his ayurvedic regime and lead normal menstrual and reproductive lives.
The basis for this new concept arose, because one case of Mullerian Dysgenesis, wherein clinically, there was no vagina but with introital depression, on imaging, there was a midline nodule without a cavity, at the normal site of the uterus and on diagnostic laparoscopy, showed two tubes arising from the upper and outer aspects of the nodule, thus proving conclusively, that it was a rudimentary uterine nodule. This nodule grew into a uterus with cavity and menstruated on using his regime ( ref. – www.mullerian-malformations.blogspot.com. & http://drecsreevalsan.blogspot.com. ). If one nodule could grow and become normal, it is only reasonable to expect others to respond.
In 2005, after getting a Patent from the Government of India entitled “ An unique combination of ayurvedic compounds for correcting a rare form of Mullerian Dysgenesis “, he started, in a modest way, “Correction of Mullerian Dysgenesis “ at A.G.Chromepet Public Health & Maternity Centre, Chromepet, Chennai as a prospective one, on 01-04-2005. According to him, since it was only a defect and not a disease, one could only attempt a correction and not a cure. The incidence of Mullerian Dysgenesis is nearly 1 %. The cause is not known.
None of the video-lap pictures show any midline uterine swelling. Of the 15 cases undergoing correction, there were 1 each in hypoplastic uterus and unilateral nodule and the remaining 13, were of bilateral nodule variety. All the cases are showing development and of these, 4 (of the bilateral nodule cases) have developed cavity and lining (genetic evolutionary response) and in 3, increased thickening of the lining (early hormonal (functional) response and therefore, it is only a matter of time, for them, to menstruate,(attain menarche), thus lending credence to the “New Concept”.
This medical option now, provides us with a correction procedure for this category of birth defect.
Key Words: Mullerian Tract Defect – Dysgenesis – Primary Amenorrhoea – Correction – Eugenesis – Normal Menstrual and Reproductive Life.
Results at a glance:
(1)Hypoplastic uterus – 1 – progressing
(2) Uni-lateral uterine nodule – 1 – Three dimensional growth.
(3) Bilateral uterine nodule - 13
(a) Pregnancy - nil
(b) Menstruation - nil
(c) Cavity & Lining - 4
(d) Cavity only - 1 (transitory)
(e) 3 dimensional - 4
(f) 2 dimensional - 4
(g) 1 dimensional - 1
(4) No Change - nil
(5) Deterioration - nil
N.B.: The unique feature of this report is that, in three cases (out of four), there has been increase in E.T. (albeit slowly) and is, obviously, evidence of response to ovarian (hormonal) stimulation, thus completing all the basic steps (page.1.), followed by the rudimentary uterine nodule before menstruation. Now it is only a matter of time (since response to ovarian hormones has started) for menarche (first menstruation) to take place.
The Second Correction Report.(01-08-2010)
Preface:
Eugenesis takes place when the genetic drive is normal. When the genetic drive is not normal either Agenesis or Dysgenesis takes place, depending on whether the genetic drive is either absent or has gone awry. There is yet one more possibility, clinically. The genetic drive is normal and eugenesis takes place but then due to unknown cause/s, Regression takes place. In Testicular Regression Syndrome, depending on when, during pregnancy (embryonic or fetal), the testicular failure commences we find clinically the external genitalia changing from feminine to ambiguous and finally to masculine (but with anorchia). Moreover, when we trace the line of Mullerian duct growth, we find discontinuity by segmental disruption. This could take place either due to segmental growth or due to segmental regression. Obviously there must be a genetic factor which maintains or regulates the genetic drive. If we can stimulate this factor, then we can expect the activation of the genetic drive in cases of Agenesis or Dysgenesis, thus resulting in the growth of absent or stunted Mullerian tissue on normal lines.
The basis for this new concept arose because one case of Mullerian Dysgenesis, wherein clinically, there was no vagina but with introital depression, on imaging, there was a nodule without a cavity at the normal site of the uterus and on diagnostic laparoscopy, showed two tubes arising from the upper and lateral aspects of the nodule, thus conclusively proving that it was a rudimentary Uterine nodule. This nodule grew into a near normal sized uterus with cavity and menstruated. If one nodule could grow and become normal, it is only reasonable to expect others to respond.
The concept of a genetic drive raises many questions:-
Why did the original genetic drive remain dormant or came to a standstill? (creating so many Anomalies – fusion & non-fusion defects – vertical and lateral )
Did regression take place after formation? (segmental loss seen)
Did development or growth take place irregularly? (irregular segments seen )
Can functional regression take place after birth? (only about 20% of female babies show withdrawal bleeding )
Can regression take place after menarche? (a few cases of secondary amenorrhoea seen with no obvious infection )
Is the genetic drive responsible for the synchronization of the HPO Axis (Ovarian cycle) and the Mullerian system (Endometrial cycle) (the ovaries are not important when determining sexual development. Moreover, when only one X is present, ovaries with follicles do develop but soon the follicles disappear leaving behind streak ovaries. Similarly, when the short arm of X chromosome is absent there is ovarian agenesis. (genetic influence)
Is premature menopause and menopause expressions of regression of genetic drive? Atrophy of Uterus which follows these conditions is a form of regression.
We cannot answer these questions now.
Let us study the steps involved in the growth of the rudimentary uterine tissue into a normal uterus with function.
The steps involved in the correction of Mullerian Dysgenesis are:-
a) Growth or development (3 dimensional) of the uterine nodule.
b) Cavity formation within it
c) Epithelium formation within the newly formed cavity and
d) Functional response to the action of the ovarian steroids resulting in menstruation.
Details of the recorded changes are given in my websites:
http://mullerian-malformation.blogspot.com/2009/05/correction-of-uterine-nodule.html
http://mullerian-malformation.blogspot.com/2009/05/correction-of-uterine-nodule.html
http://drecsreevalsan.blogspot.com/
Can a birth defect like Mullerian Dysgenesis be corrected?
You will get the answer to this question, when you have read this report in its entirety. Please proceed.
It is the training obtained at the Govt. College of Integrated Medicine, which made the undersigned employ Ayurvedic Compounds ( since Allopathy had no medical option ) and ensure that the necessary proof ( serial USG Scans ) was available throughout the course of correction and has presented the facts for easy understanding of one and all. This medical option (as there is no medical option in any system of medicine for this condition and is in a state of equipoise) is only a small step in the unraveling of nature’s mystery. This will provide a whole generation of investigators – clinicians, phytochemists, geneticists etc., enough material and help evaluation of all aspects of this option. This medical option is being used to correct other cases as and when they come, after all relevant investigations. What follows, is the results of 12 months of correction and you can decide whether the first step of correction, namely, growth has been achieved or not
.
Introduction.
The correction of Mullerian Dysgenesis was started at A.G.Chromepet Public Health & Maternity Centre, Chromepet, and Chennai.600044. as a prospective one, on 01 – 04 – 2005. From 26-07-2009 till 31-07-2010, 35 cases of amenorrhoea ( 34 primary and 1 secondary ) were seen in O.P. practice at A.G.Hospital, which is a primary, non-teaching, semi-urban hospital.
The salient features of the correction are as follows:-
On the first appointment day, blood is taken for Karyotyping, Hormonal estimation and other routine tests. Urine routine tests are also done. A clinical examination after taking a detailed history is done and then patient is sent for an USG Scan. When the Karyotype report comes, if she is 46, XX, a diagnostic video-laparoscopy is done and findings recorded. Cases of Karyotype other than 46, XX, are not taken up for further tests. If the scan shows absence of ovaries, she is sent for an MRI and if ovaries are present, she is taken up for correction. If no ovaries are visualized in the MRI, she is not taken up for correction.
Patients, taken up for correction, are given one month’s medicine and they are asked to come every month for scan and medicine. Every third month hormonal estimation and physical examination done and progress noted. Physical examination done as and when patient has any specific complaint, to reassure her and to detect cause.
The Ayurvedic Regime consists of 11 compounds given in 8 phases and the phases are for different durations. When a scan showed increase of any dimension by 0.5 centimetre or more it was regarded as progress and the next phase of the regime brought forward. Karyotyping revealed 5 cases of Turner’s Syndrome, 1 case of 46, XY, and 1 case of Triple X Syndrome Mosaic and remaining 28 cases were 46, XX, of whom 7 had additional features.
The 7 cases which had additional features were as follows:-
(a) mos 46, XX, t(1;3)(1p34.1;3p21) – translocation of chromosome 1p34.1;3p21 in 60% of cells. (1p34.1;3p21) karyotype has been reported with reproductive failure in both men and women. This case has not reported for further evaluation.
(b) 46, XX, ins(2q)(11.1;21.2) mosaic in 20% of cells. This case has reported and correction started.
(c) 46, XX, ins (7p)(p21;p14) mosaic in 20% of cells She has not reported till date.
(d) Mos 46, XX, del (xy) (q25; q28) in 14 % of cells. She is yet to report.
(e) 46, XX, add (22) (p13) in all the cells. She is undergoing correction.
(f) 46 X, IsoX, 14p+ in all the cells.
(g) 46, XX, inv (9) (p.11q13) (not associated with any abnormal condition)
Of these 28 cases, 21 underwent further analysis viz. Diagnostic Video-Laparoscopy. Of these 21 cases, 2 underwent M.R.I. and 1 of them was a case of Ovarian Agenesis (Mosaic Triple X). 20 cases are now undergoing correction.
Pre-correction Evaluation :-
Under normal circumstances, this anatomical defect (absence of uterus and/or vagina) will present as primary amenorrhoea around the age of 16 years and is now being studied under three heads:-
(a)Medical aspect
(b)Palm Print aspect and
(c)Natal Chart aspect
(a )Medical aspect:-is based mainly on the findings of both imaging and diagnostic video-laparoscopy and the following categories were encountered;

(b) Palm Print Aspect :( based on a report by Dr. Arunachalam Kumar that “ Open Fields “ over the thenar eminences was indicative of Mullerian Agenesis ). In 13 cases there were “ Open Fields “ bilaterally, in 2 cases on the right only, in 2 cases on the left only and in 3 cases there were no “ Open Fields “ at all.
( c ) Natal Chart Aspect: ( According to an astrological aphorism, if in the natal chart, the seventh house is owned by Sun, Mars or Saturn and the seventh lord is posited in the house of Sun, Mars or Saturn in Navamsa and not viewed by benefics, such an individual is likely to have a defective generative tract. ) Of the 20 natal charts available for study, it was found that 4 were strongly positive, 9 were positive, 1 was weakly positive and 6 were negative.
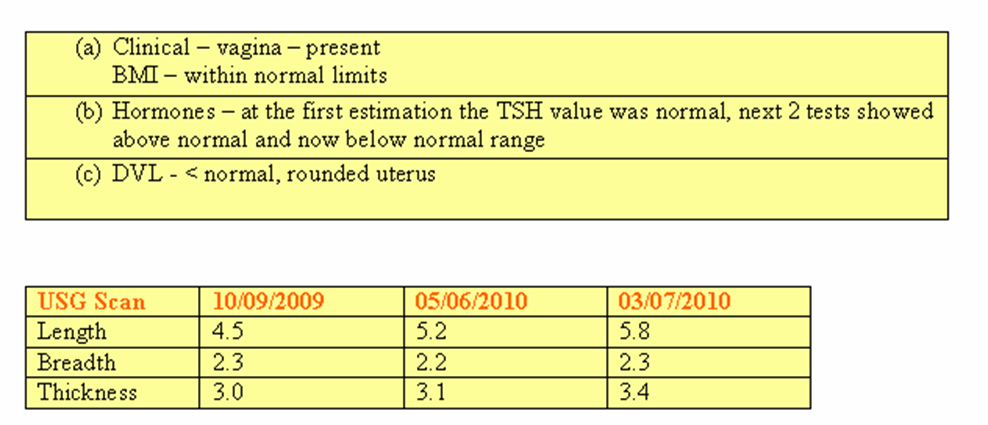
A. Clinical Evaluation.(including family history and relevant earlier reports)
(a) Age :In the group 14-16, there were 5 cases, 3 cases in group 17-19 but the majority, 12 were in group 20-39.
(b) Height : There were 4 cases in group 150 cms. & below and the remaining 16 were above 150 cms.
(c) Body Mass Index or Quetelet Index: ( normal range – 19 – 28 ) There were 15 cases who were normal and the rest underweight.
(d) There was no obvious case of goiter or hirsutism.
(e) There were no case of discharge from the nipples and Tanner staging of the breasts showed 3 cases in stage 3, 3 cases in stage 4 and the remaining 14 were in stage 5.
(f) As regards hair, - in the axillae, there was 1 case of stage 1, 3 cases in stage 2 and the remaining 16 were in stage 3. In the pubic region, there was 1 case of stage 4 and the rest (19) were in stage 5.
(g) External genitalia examination did not reveal any case of fused labia. Vagina was present in 11 cases, 5 showed introital depression and in 4 cases there were no suggestion of a vagina.
(h) Vaginal examination was done in 4 cases, who were married and it revealed (i) a hypoplastic uterus in the midline, (ii) a left unicornuate uterus with cervical aplasia ( vaginal aplasia corrected by vaginoplasty ), (iii) a left sided hypoplastic uterus and (iv) a midline uterine nodule.
(i) Rectal examination: In 10 cases no uterine nodule was palpable and in the remaining 10 uterii or uterine nodules were palpable.
(j) Family History: 4 cases were married and the remaining 16 were single. None of them had attained menarche. One case had withdrawal bleeding from the age of 15 for 8 years. She stopped medication 8 years ago and since then has not had any vaginal bleeding. The others did not respond to any medication. There was no case of delayed menarche in any other family member and no other member had a similar complaint.
(k) Associated Anomaly : 1 case had associated congenital anomaly of the cervical vertebrae and had partial loss of hearing.
B. Blood Tests :
(1) Group & Type : Of these 11 - cases were ‘ O ‘, 3 - cases were ‘ A ‘ and the remaining 6 - cases were ‘B’. There was one case of Rh negative and the others were Rh positive.
(2) General -
(a) Blood.
(i) Haemoglobin : The least was 10 and the highest was 13.
(ii) Packed Cell Volume : This ranged between 31 and 40.
(iii) Other parameters were within normal limits.
(b) Urine: There were no specific changes in the urine except aciduria in all cases.
(3) Specific - Hormones : The following hormones – Estrogen, Progesterone, FSH, LH, Testosterone, Prolactin, T 3,T 4 and TSH were tested once in three months. In eleven cases initially values of some hormones were either below or above normal limits but they subsequently became normal except in one case where TSH was normal to begin with, but subsequently went above normal and finally went below normal. The conclusion from this is that one test of hormones is not final. Pre-menarcheal hormones have not been studied exhaustively and one cannot arrive at any standard. This correction regime is likely to enhance our knowledge in this respect as this is a prospective one and we are dealing with the anatomical cause of primary amenorrhoea and it may help us understand the relationship between hormones and menstruation ( as we are continuously monitoring the growth of the uterine nodule.) Mention will be made about the individual changes during the category-wise report.
USG Scans is not only our basic investigatory modality but also our follow-up method to assess the primary problem and its progress during correction, although one has to admit that menstruation is the true proof of success.
Diagnostic Video-Laparoscopy is another basic investigatory modality based on which the initial selection of cases is done and those with no ovaries are rejected forthwith. D.V.L. revealed 1 case of pelvic kidney, 1 case of round ligaments entering sacs prior to entry into inguinal canal, 1 case without tubes, 1 case of rudimentary tube with the contra-lateral one being normal, 1 tube ending bluntly with no fimbria. It also revealed 16 bilateral uterine nodules, 1 unilateral uterine nodule, 2 hypoplastic uteri and 1 unilateral, uni-cornuate, normal uterus with regurgitation of menstrual fluid.
MRI was resorted in 2 cases – the first one showed absence of both uterus and ovaries in the USG Scan and the MRI revealed ovaries and hence patient taken up for correction and in the second case there were no ovaries at all and hence rejected.
Evaluation during Correction.
Before we discuss evaluation one thing must be made clear. In Ayurveda correction is always based on the individual’s constitution. In other words, correction is never generalized. Therefore, we will find, occasionally, lack of sufficient progress when we give a regime of drugs. Moreover, as the BMI improves, we will find progressive development. In other words, only if the patient is physically fit or becoming fit progressively, you are likely to note improvement. The first USG Scan (on admission) and the last two scan reports before 31 – 07 – 2010 are given for comparison to show the changes in measurements of the uterus/ uterine nodule/s. An increase of 0.5 centimeters and more in any dimension in the scan report is considered as growth or development.
Now, we shall analyse the cases according to the categories mentioned earlier.
[ Click Tables for Magnification ]
[ Click Tables for Magnification ]

CATEGORY – 1
Normal Uterus with Cervical & Vaginal Aplasia – 1 case.
Patient was a married woman with primary amenorrhoea and history of vaginoplasty before marriage and had a left-sided unicornuate uterus with absent cervix on USG Scan. During Diagnostic Video-Laparoscopy. Regurgitation of blood was seen from the left tube into the peritoneal cavity.
Cervical reconstruction and utero-vaginal anastomosis was done and she had her next period per via naturalis during the post-operative phase.

N.B. After reconstruction, the length of the uterus has increased.

CATEGORY – 2
Hypoplastic Uterus ( 1 in midline & another 1 on left side )
Midline uterus case – period of correction – 11 months.

Left Sided Hypoplastic Uterus – Period of Correction – 9 months


CATEGORY – 3. Bilateral Uterine Nodules – 16
Period of correction:
a) 12 months – 2cases
b) 11 months - 1 case
c) 9 months - 4 cases
d) 8 months - 2 cases
e) 6 months – 1 case
f) 5 months – 1 case
g) 4 months – 2 cases
h) 3 months – 2 cases
i) 2 months – 1 case
(a) 2 cases
(1)



(c)4 cases – (1),(2),(3),(4)
(1)

N.B: Patient was irregular in attendance and has not reported for correction after April







Results at a glance:-
Category– 1 (1 case) – a normal uterus with cervical aplasia – outflow
tract corrected surgically. Now, one has to wait for
spontaneous regular menstruation or pregnancy.
Category –2 (2 cases) – hypoplastic uteri
(a) Length increased by 1.3 cms.(correction – 11 months)
(b) Only marginal growth noted.(correction – 9 months)
Category – 3 (16 cases) – bilateral uterine nodules
12 months (correction) – 2 cases.
(a) no change
(b) increase of thickness by 1.0 cms.
11 months (correction) – 1 case
uterus not seen – 3 dimensional growth
9 months (correction) – 4 cases
(a) only marginal change
(b) breadth increased by 0.5cms.
(c) uterus not seen – 3 dimensional growth
(d) uterus not seen – 3 dimensional growth
8 months (correction) - 2 cases
(a) The measurements showed a downward trend, but
the final scan showed E.T.2m.m. indicating that cavity and lining had formed.
(b) Showed an increase of 0.5 cms.
6 months (correction) – 1 case
Showed only marginal increase
5 months (correction) 1 case
Length increased by 1.2 cms and thickness by0.9 cms
4 months (correction) 2 cases
(a) Length increased by 0.6 cms.
(b) showed increase in all measurements
3 months (correction) 2 cases
(a) uterus not seen – 3 dimensional growth from the very next month of correction
(b) length increase by 0.5 cms.
2 months (correction) 1 case
Breadth increase by 0.6 cms. and
Thickness increase by 0.7 cms.
Category – 4 (1 case). – unilateral nodule (right )
Uterus not seen – 3 dimensional growth
N.B.: There were 5 cases of no uterus seen on initial scan
and all of them showed 3 dimensional growth subsequently.
3. Bilateral Uterine Nodules
(b)
Growth (correction) Graph

(C) (4)
Growth (correction) Graph

N.B. Correction started the very next month.
4. Unilateral Uterine Nodule.
Growth (correction) Graph

The reader, now, having been convinced by the spectacular
growth that has been registered, will be wondering how a peer
review of this report can take place and will feel that it is well nigh
impossible for two obvious reasons. The first one is, of course, the
absence of an allopathic and an ayurvedic doctor on the editorial
panel of a journal and the second one being that the correction is
based on the patent obtained by the practitioner and therefore the
ayurvedic doctor will not be able to comment on the ayurvedic
aspects of the compounds (unpublished) used for the correction.
It may seem needless to stress that this is the first medical
option available for this condition but as this condition has an
incidence of nearly 1 % and also has a worldwide distribution, one
can very well imagine the impact.
The first case took nearly 10 years to develop into a normal
uterus and it is heartening to find that, within a year, there has been
so much improvement..
Q. E. D.
Thank you. A Quotation comes to my mind.
“THERE IS NO GREATER SIGN OF IGNORANCE THAN BELIEVING THAT THE INEXPLICABLE IS IMPOSSIBLE”.
.BILARD
.BILARD

Thank You




